Tips On How To Address Pes Planus
Overview

The appearance of flat feet is normal and common in infants, partly due to "baby fat" which masks the developing arch and partly because the arch has not yet fully developed. The human arch develops in infancy and early childhood as part of normal muscle, tendon, ligament and bone growth. Training of the feet, especially by foot gymnastics and going barefoot on varying terrain, can facilitate the formation of arches during childhood, with a developed arch occurring for most by the age of four to six years. Flat arches in children usually become proper arches and high arches while the child progresses through adolescence and into adulthood.
Causes
Infants and young children naturally have flat feet. The arch should develop over time. Sometimes, the arch does not develop. It is not always clear why this happens. Flat feet may develop because of ruptured or damaged tendon that supports the arch, medical conditions that affect muscles or nerves in the foot, degenerative changes in certain foot joints, Ligament damage in the foot.
Symptoms
Arches can be seen as ?rolling downward? or collapsing when walking. Pain may present in lower back, hips or knees. Pain may be present on the bottom of the heels, within the arch, within the ankles or even the forefoot. Swelling can occur. Pain may occur in the anterior leg muscles.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
heelsncleavage
Non Surgical Treatment
There are home remedies to prevent or manage pain from fallen arches or flat feet. Here are some areas to consider. Wear footwear or shoe inserts that are appropriate to your activity. When pain occurs, try at-home treatment of rest, ice, and over-the-counter nonsteroidal anti-inflammatories, or NSAIDS, such as ibuprofen. Ask your doctor or a physical therapist to show you stretches that can prepare you for feet-intensive activities. Limit or treat risk factors that can make fallen arches or flat feet worse, such as diabetes, high blood pressure, and obesity. Avoid activities that put excessive stress on your feet, such as running on roads. Avoid high-impact sports such as basketball, hockey, soccer, and tennis. Know when to get help. When pain is severe or interferes with activities, it's time to see the doctor for a thorough exam and treatment.
Surgical Treatment

This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
The appearance of flat feet is normal and common in infants, partly due to "baby fat" which masks the developing arch and partly because the arch has not yet fully developed. The human arch develops in infancy and early childhood as part of normal muscle, tendon, ligament and bone growth. Training of the feet, especially by foot gymnastics and going barefoot on varying terrain, can facilitate the formation of arches during childhood, with a developed arch occurring for most by the age of four to six years. Flat arches in children usually become proper arches and high arches while the child progresses through adolescence and into adulthood.
Causes
Infants and young children naturally have flat feet. The arch should develop over time. Sometimes, the arch does not develop. It is not always clear why this happens. Flat feet may develop because of ruptured or damaged tendon that supports the arch, medical conditions that affect muscles or nerves in the foot, degenerative changes in certain foot joints, Ligament damage in the foot.
Symptoms
Arches can be seen as ?rolling downward? or collapsing when walking. Pain may present in lower back, hips or knees. Pain may be present on the bottom of the heels, within the arch, within the ankles or even the forefoot. Swelling can occur. Pain may occur in the anterior leg muscles.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
heelsncleavage
Non Surgical Treatment
There are home remedies to prevent or manage pain from fallen arches or flat feet. Here are some areas to consider. Wear footwear or shoe inserts that are appropriate to your activity. When pain occurs, try at-home treatment of rest, ice, and over-the-counter nonsteroidal anti-inflammatories, or NSAIDS, such as ibuprofen. Ask your doctor or a physical therapist to show you stretches that can prepare you for feet-intensive activities. Limit or treat risk factors that can make fallen arches or flat feet worse, such as diabetes, high blood pressure, and obesity. Avoid activities that put excessive stress on your feet, such as running on roads. Avoid high-impact sports such as basketball, hockey, soccer, and tennis. Know when to get help. When pain is severe or interferes with activities, it's time to see the doctor for a thorough exam and treatment.
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Functional Leg Length Discrepancy Way Of Measuring
Overview
Approximately 75% of us present with one leg longer than the other. It?s staggering, literally, that so many people walk about with an imbalance. Yet to have one leg longer than the other doesn?t seem to create pain for everyone but for those that it does it brings pain in a myriad of dysfunction from TMJ, headaches, low back pain, IBS, bladder problems, sexual dysfunction, sacroiliac joint pain, pubis dysfunction, groin strain, gluteal dysfunction as well as the formation of trigger points.
Causes
Some children are born with absence or underdeveloped bones in the lower limbs e.g., congenital hemimelia. Others have a condition called hemihypertrophy that causes one side of the body to grow faster than the other. Sometimes, increased blood flow to one limb (as in a hemangioma or blood vessel tumor) stimulates growth to the limb. In other cases, injury or infection involving the epiphyseal plate (growth plate) of the femur or tibia inhibits or stops altogether the growth of the bone. Fractures healing in an overlapped position, even if the epiphyseal plate is not involved, can also cause limb length discrepancy. Neuromuscular problems like polio can also cause profound discrepancies, but thankfully, uncommon. Lastly, Wilms? tumor of the kidney in a child can cause hypertrophy of the lower limb on the same side. It is therefore important in a young child with hemihypertrophy to have an abdominal ultrasound exam done to rule out Wilms? tumor. It is important to distinguish true leg length discrepancy from apparent leg length discrepancy. Apparent discrepancy is due to an instability of the hip, that allows the proximal femur to migrate proximally, or due to an adduction or abduction contracture of the hip that causes pelvic obliquity, so that one hip is higher than the other. When the patient stands, it gives the impression of leg length discrepancy, when the problem is actually in the hip.
Symptoms
The symptoms of limb deformity can range from a mild difference in the appearance of a leg or arm to major loss of function of the use of an extremity. For instance, you may notice that your child has a significant limp. If there is deformity in the extremity, the patient may develop arthritis as he or she gets older, especially if the lower extremities are involved. Patients often present due to the appearance of the extremity (it looks different from the other side).
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
In some circumstances, the physician will recommend a non-surgical form of treatment. Non-surgical treatments include orthotics and prosthetics. Orthotics are a special type of lift placed in or on a shoe that can be used in the treatment of leg length discrepancies between two and six centimeters. In pediatric patients who have large discrepancies and are not good candidates for other treatment forms, prosthetics can be helpful.

leg length discrepancy symptoms
Surgical Treatment
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Approximately 75% of us present with one leg longer than the other. It?s staggering, literally, that so many people walk about with an imbalance. Yet to have one leg longer than the other doesn?t seem to create pain for everyone but for those that it does it brings pain in a myriad of dysfunction from TMJ, headaches, low back pain, IBS, bladder problems, sexual dysfunction, sacroiliac joint pain, pubis dysfunction, groin strain, gluteal dysfunction as well as the formation of trigger points.
Causes
Some children are born with absence or underdeveloped bones in the lower limbs e.g., congenital hemimelia. Others have a condition called hemihypertrophy that causes one side of the body to grow faster than the other. Sometimes, increased blood flow to one limb (as in a hemangioma or blood vessel tumor) stimulates growth to the limb. In other cases, injury or infection involving the epiphyseal plate (growth plate) of the femur or tibia inhibits or stops altogether the growth of the bone. Fractures healing in an overlapped position, even if the epiphyseal plate is not involved, can also cause limb length discrepancy. Neuromuscular problems like polio can also cause profound discrepancies, but thankfully, uncommon. Lastly, Wilms? tumor of the kidney in a child can cause hypertrophy of the lower limb on the same side. It is therefore important in a young child with hemihypertrophy to have an abdominal ultrasound exam done to rule out Wilms? tumor. It is important to distinguish true leg length discrepancy from apparent leg length discrepancy. Apparent discrepancy is due to an instability of the hip, that allows the proximal femur to migrate proximally, or due to an adduction or abduction contracture of the hip that causes pelvic obliquity, so that one hip is higher than the other. When the patient stands, it gives the impression of leg length discrepancy, when the problem is actually in the hip.
Symptoms
The symptoms of limb deformity can range from a mild difference in the appearance of a leg or arm to major loss of function of the use of an extremity. For instance, you may notice that your child has a significant limp. If there is deformity in the extremity, the patient may develop arthritis as he or she gets older, especially if the lower extremities are involved. Patients often present due to the appearance of the extremity (it looks different from the other side).
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
In some circumstances, the physician will recommend a non-surgical form of treatment. Non-surgical treatments include orthotics and prosthetics. Orthotics are a special type of lift placed in or on a shoe that can be used in the treatment of leg length discrepancies between two and six centimeters. In pediatric patients who have large discrepancies and are not good candidates for other treatment forms, prosthetics can be helpful.
leg length discrepancy symptoms
Surgical Treatment
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Coping with Mortons Neuroma
Overview
 Morton's neuroma is the common name given to the nerve irritation that is found in the ball of the foot that may or may not be accompanied by an inter-metatarsal bursae (a bursa-neuromal complex). It is often associated with inflammation or degeneration and often occurs with constant pressure or irritation of the nerve from the surrounding bony structures or local bursas (fluid filled sacs). Morton's Neuroma can cause symptoms such as a sharp pain, burning even a lack of feeling in the ball of the foot and associated toes.
Morton's neuroma is the common name given to the nerve irritation that is found in the ball of the foot that may or may not be accompanied by an inter-metatarsal bursae (a bursa-neuromal complex). It is often associated with inflammation or degeneration and often occurs with constant pressure or irritation of the nerve from the surrounding bony structures or local bursas (fluid filled sacs). Morton's Neuroma can cause symptoms such as a sharp pain, burning even a lack of feeling in the ball of the foot and associated toes.
Causes
The source of this pain is an enlargment of the sheath of an intermetatarsal nerve in the foot. This usually occurs in the third intermetatarsal space, the space between the third and fourth toes and metatarsals. It occurs here, at the site third intermetatarsal nerve, since this intermetatarsal nerve is the thickest being comprised of the joining of two different nerves. It also may occur in the other intermetatarsal areas, with the second interspace being the next most common location.
Symptoms
Patients will often experience a clicking feeling in the forefoot followed by a sharp shooting pain or a sensation of numbness or pins and needles extending into ends of their toes. Tight narrow fitting shoes may often exacerbate these feelings which become worse after long periods of standing or walking. Once the Mortons nueroma progresses symptoms will become more frequent and often more intense.
Diagnosis
Diagnosis of Morton?s Neuroma typically involves a physical examination of the affected foot. Your health care provider will ask you about your symptoms and examine your feet and toes. He will manipulate your toes, pushing them from side to side and squeezing on the spaces in between. This physical exam will allow your health care provider to feel for any lumps that may be present under the soft tissue of your feet. Your health care provider may also listen for any clicking sounds that your bones may be making. Known as Muldor?s Sign, this clicking is common amongst sufferers of foot neuroma. Occasionally, an x-ray or MRI (magnetic resonance imaging) is performed to help rule out any breaks, sprains, or fractures in your foot.
Non Surgical Treatment
Once a diagnosis is obtained, it is essential to begin treatment immediately. Your podiatric physician will advise you on the most effective means. If caught early enough, good foot care, shoes that fit properly, and/or orthoses may eliminate the need for any further intervention. Other conservative measures might include oral non-steroidal anti-inflammatory medication (NSAIDS), physical therapy, ultrasound or other non-invasive measures. If that doesn?t work, your podiatric physician might use injectable steroids, and/or a local anesthetic around the neuroma to reduce inflammation and pain. Many patients report relief after these measures are taken.
Surgical Treatment
For severe or persistent pain, you may need surgery to remove the neuroma. Once the nerve is gone, you permanently lose feeling in the affected area. One alternative to surgery is to undergo neurolysis injections. These use chemical agents to block pain signals. Another alternative is to take a prescription pain reliever that alleviates nerve pain.
Morton's neuroma is the common name given to the nerve irritation that is found in the ball of the foot that may or may not be accompanied by an inter-metatarsal bursae (a bursa-neuromal complex). It is often associated with inflammation or degeneration and often occurs with constant pressure or irritation of the nerve from the surrounding bony structures or local bursas (fluid filled sacs). Morton's Neuroma can cause symptoms such as a sharp pain, burning even a lack of feeling in the ball of the foot and associated toes.Causes
The source of this pain is an enlargment of the sheath of an intermetatarsal nerve in the foot. This usually occurs in the third intermetatarsal space, the space between the third and fourth toes and metatarsals. It occurs here, at the site third intermetatarsal nerve, since this intermetatarsal nerve is the thickest being comprised of the joining of two different nerves. It also may occur in the other intermetatarsal areas, with the second interspace being the next most common location.
Symptoms
Patients will often experience a clicking feeling in the forefoot followed by a sharp shooting pain or a sensation of numbness or pins and needles extending into ends of their toes. Tight narrow fitting shoes may often exacerbate these feelings which become worse after long periods of standing or walking. Once the Mortons nueroma progresses symptoms will become more frequent and often more intense.
Diagnosis
Diagnosis of Morton?s Neuroma typically involves a physical examination of the affected foot. Your health care provider will ask you about your symptoms and examine your feet and toes. He will manipulate your toes, pushing them from side to side and squeezing on the spaces in between. This physical exam will allow your health care provider to feel for any lumps that may be present under the soft tissue of your feet. Your health care provider may also listen for any clicking sounds that your bones may be making. Known as Muldor?s Sign, this clicking is common amongst sufferers of foot neuroma. Occasionally, an x-ray or MRI (magnetic resonance imaging) is performed to help rule out any breaks, sprains, or fractures in your foot.
Non Surgical Treatment
Once a diagnosis is obtained, it is essential to begin treatment immediately. Your podiatric physician will advise you on the most effective means. If caught early enough, good foot care, shoes that fit properly, and/or orthoses may eliminate the need for any further intervention. Other conservative measures might include oral non-steroidal anti-inflammatory medication (NSAIDS), physical therapy, ultrasound or other non-invasive measures. If that doesn?t work, your podiatric physician might use injectable steroids, and/or a local anesthetic around the neuroma to reduce inflammation and pain. Many patients report relief after these measures are taken.
Surgical Treatment
For severe or persistent pain, you may need surgery to remove the neuroma. Once the nerve is gone, you permanently lose feeling in the affected area. One alternative to surgery is to undergo neurolysis injections. These use chemical agents to block pain signals. Another alternative is to take a prescription pain reliever that alleviates nerve pain.
Are Shoe Lifts The Answer To Leg Length Difference
There are not one but two unique variations of leg length discrepancies, congenital and acquired. Congenital means that you are born with it. One leg is anatomically shorter in comparison to the other. As a result of developmental stages of aging, the brain picks up on the step pattern and recognizes some difference. The body typically adapts by tilting one shoulder over to the "short" side. A difference of less than a quarter inch isn't grossly abnormal, doesn't need Shoe Lifts to compensate and mostly does not have a serious effect over a lifetime.

Leg length inequality goes mainly undiagnosed on a daily basis, yet this problem is easily remedied, and can eradicate many cases of back discomfort.
Treatment for leg length inequality typically involves Shoe Lifts. These are typically economical, typically being below twenty dollars, compared to a custom orthotic of $200 if not more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is the most common condition afflicting men and women today. Over 80 million people have problems with back pain at some point in their life. It is a problem which costs employers millions of dollars year after year as a result of time lost and productivity. Innovative and superior treatment methods are always sought after in the hope of reducing the economical influence this condition causes.

People from all corners of the earth suffer from foot ache due to leg length discrepancy. In a lot of these cases Shoe Lifts might be of very beneficial. The lifts are capable of eliminating any pain and discomfort in the feet. Shoe Lifts are recommended by countless specialist orthopaedic physicians.
So that you can support the body in a healthy and balanced fashion, the feet have a critical task to play. In spite of that, it is often the most neglected zone in the human body. Many people have flat-feet meaning there is unequal force placed on the feet. This will cause other parts of the body like knees, ankles and backs to be impacted too. Shoe Lifts ensure that suitable posture and balance are restored.
Leg length inequality goes mainly undiagnosed on a daily basis, yet this problem is easily remedied, and can eradicate many cases of back discomfort.
Treatment for leg length inequality typically involves Shoe Lifts. These are typically economical, typically being below twenty dollars, compared to a custom orthotic of $200 if not more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is the most common condition afflicting men and women today. Over 80 million people have problems with back pain at some point in their life. It is a problem which costs employers millions of dollars year after year as a result of time lost and productivity. Innovative and superior treatment methods are always sought after in the hope of reducing the economical influence this condition causes.
People from all corners of the earth suffer from foot ache due to leg length discrepancy. In a lot of these cases Shoe Lifts might be of very beneficial. The lifts are capable of eliminating any pain and discomfort in the feet. Shoe Lifts are recommended by countless specialist orthopaedic physicians.
So that you can support the body in a healthy and balanced fashion, the feet have a critical task to play. In spite of that, it is often the most neglected zone in the human body. Many people have flat-feet meaning there is unequal force placed on the feet. This will cause other parts of the body like knees, ankles and backs to be impacted too. Shoe Lifts ensure that suitable posture and balance are restored.
Painless Hammertoe Surgery
 Overview
Overview
There are two different types. Flexible Hammer toe. These are less serious because they can be diagnosed and treated while still in the developmental stage. They are called flexible hammertoes because they are still moveable at the joint. Rigid Hammertoes. This variety is more developed and more serious than the flexible condition. Rigid hammertoes can be seen in patients with severe arthritis, for example, or in patients who wait too long to seek professional treatment. The tendons in a rigid hammertoe have become tight, and the joint misaligned and immobile, making surgery the usual course of treatment.
Causes
Your shoes, your genetic predisposition, an underlying medical condition or all of these can make you susceptible to developing one of Hammer toe these deformities of the toes. The genes your parents gave you. When it comes to genetics, the foot type you?re born with predisposes you to developing this type of joint deformity over a lifetime. For many, a flat flexible foot leads to hammertoes as the foot tries to stabilize against a flattening arch. Those with high arches can also form hammertoes as the extensor tendons overpower the flexors.
 Symptoms
Symptoms
People who have painful hammertoes visit their podiatrist because their affected toe is either rubbing on the end their shoe (signaling a contracted flexor tendon), rubbing on the top of their shoe (signaling a contracted extensor tendon), or rubbing on another toe and causing a painful buildup of thick skin, known as a corn.
Diagnosis
The exam may reveal a toe in which the near bone of the toe (proximal phalanx) is angled upward and the middle bone of the toe points in the opposite direction (plantar flexed). Toes may appear crooked or rotated. The involved joint may be painful when moved, or stiff. There may be areas of thickened skin (corns or calluses) on top of or between the toes, a callus may also be observed at the tip of the affected toe beneath the toenail. An attempt to passively correct the deformity will help elucidate the best treatment option as the examiner determines whether the toe is still flexible or not. It is advisable to assess palpable pulses, since their presence is associated with a good prognosis for healing after surgery. X-rays will demonstrate the contractures of the involved joints, as well as possible arthritic changes and bone enlargements (exostoses, spurs). X-rays of the involved foot are usually performed in a weight-bearing position.
Non Surgical Treatment
Conservative treatment starts with new shoes that have soft, roomy toe boxes. Shoes should be one-half inch longer than your longest toe. For many people, the second toe is longer than the big toe.) Avoid wearing tight, narrow, high-heeled shoes. You may also be able to find a shoe with a deep toe box that accommodates the hammer toe. Or, a shoe repair shop may be able to stretch the toe box so that it bulges out around the toe. Sandals may help, as long as they do not pinch or rub other areas of the foot.
Surgical Treatment
If you are unable to flex your toe, surgery is the only option to restore movement. Surgery is used to reposition the toe, remove deformed or injured bone, and realign your tendons. Surgery is normally done on an outpatient basis, so you can return home on the day of your surgery.
What Are The Solutions For Bunions?
Overview
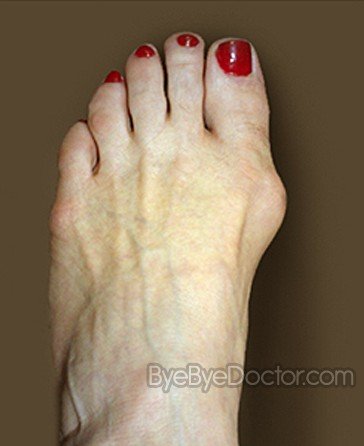 A bunion, also known by its medical name hallux abductovalgus, is foot condition in which your big toe points toward your second toe, causing a bump or prominence to develop on the inside edge of your big toe and first metatarsal bone. Your first metatarsal bone is the long bone located directly behind your big toe, in your mid-foot. A bunion will cause your forefoot to appear wider because the base of your big toe now points away from your foot instead of pointing straight ahead.
A bunion, also known by its medical name hallux abductovalgus, is foot condition in which your big toe points toward your second toe, causing a bump or prominence to develop on the inside edge of your big toe and first metatarsal bone. Your first metatarsal bone is the long bone located directly behind your big toe, in your mid-foot. A bunion will cause your forefoot to appear wider because the base of your big toe now points away from your foot instead of pointing straight ahead.
Causes
Prolonged pressure against the inside portion of the 1st MTP joint can lead to Bunions. This most commonly occurs as a result of wearing pointed toe shoes or shoes that are too tight. Another cause is over-pronation. Normal ?toe-off?occurs from bottom of the big toe. Over-pronation can cause one to ?toe-off? on the inside portion of the big toe versus the bottom. Over time, there is a retrograde force into the joint which pushes it out stretches the joint capsule. This tearing and stretching of the joint capsule as well as the wear and tear on the cartilage is what causes the pain.
Symptoms
The symptoms of bunions include irritated skin around the bunion, pain when walking, joint redness and pain, and possible shift of the big toe toward the other toes. Blisters may form more easily around the site of the bunion as well. Having bunions can also make it more difficult to find shoes that fit properly; bunions may force a person to have to buy a larger size shoe to accommodate the width the bunion creates. When bunion deformity becomes severe enough, the foot can hurt in different places even without the constriction of shoes because it then becomes a mechanical function problem of the forefoot.
Diagnosis
People with bunions may be concerned about the changing appearance of their feet, but it is usually the pain caused by the condition that leads them to consult their doctor. The doctor will evaluate any symptoms experienced and examine the affected foot for joint enlargement, tissue swelling and/or tenderness. They will also assess any risk factors for the condition and will ask about family history. An x-ray of the foot is usually recommended so that the alignment of big toe joint can be assessed. This would also allow any other conditions that may be affecting the joint, such as arthritis, to be seen.
Non Surgical Treatment
Podiatrists will treat bunions conservatively, using paddings and orthotics, which are devices that are made to protect the joint or deviate pressure away from it. Sometimes bunions will develop overlying callus or corns. These can be removed by a podiatrist, but if the area is irritated again by wearing ill-fitting footwear, the corn will grow back. Most people with this condition have flat feet, so arch supports are often recommended. 
Surgical Treatment
Bunion surgery is most often a day case or one night in hospital. Surgery can be done under ankle block (patient awake) or general anaesthetic. It is best to rest with the foot elevated for the first 2 weeks after surgery. The foot is bandaged and a special sandal supplied by the hospital is worn for 6 weeks. Sensible shoes are to be worn for a further 6 weeks after the bandages are removed. It will take between 3-6 months for the swelling to go down. It will take 12 months before everything completely settles. It is also important to remember that not all bunion operations are entirely successful.